This is a commonly performed arthroscopic shoulder operation. The aim is to increase the amount of room between the deep rotator cuff tendons of the shoulder (suprapsinatus tendon) and the overlying shoulder tip bone (acromion) and ligament (CA or CoracoAcromial ligament) and also clear any inflammation (bursitis). An ASD is not used as a first line treatment and should only be considered in selected patients after failed attempts at non-operative treatment options including physiotherapy and injections.
The operation is usually performed under general anaesthetic (GA) as a daycase procedure so patients go home on the same day.
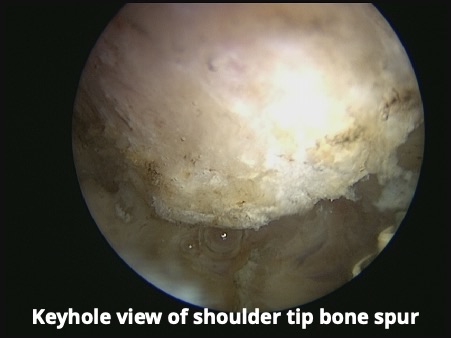
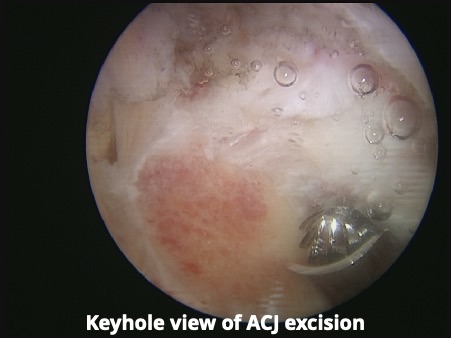
An arthroscope (keyhole camera) is inserted into the shoulder joint from the back of the shoulder. All of the anatomical structures inside the shoulder can be visualised and inspected to detect any other possible causes of symptoms. This allows the deep surface of all the rotator cuff tendons, in particular the supraspinatus tendon, to be viewed. The arthoscope is then inserted above the supraspinatus rotator cuff tendon and into the fluid filled sack underneath the shoulder tip called the subacromial bursa. Inflammation within the bursa (bursitis) can be confirmed as it will look red and thickened. The bursa and inflamed tissues are then excised (bursectomy) using a radiofrequency probe (this is a device which delivers high frequency electrical current through tissue immediately in front of the probe which is used either to cut tissue or seal bleeding blood vessels). The probe is inserted via a small incision from the side of the shoulder. The coraco-acromial ligament is also released from the front of the acromion to increase the amount of space for the tendons to move in. A high speed shaver (burr) is then inserted to excise the bone spur on the undersurface of the acromion (shoulder tip bone) and thereby prevent the spur or downsloping of the acromion bone from irritating the supraspinatus tendon below it.
You will wake up after your operation with a sling on your arm and you will wear this for 2-3 days until you feel you can move your shoulder comfortably. However, it is advisable to wear the sling if you are out in public places (shopping etc) for several weeks to try and prevent your arm being knocked or jolted.
Usually the anaesthetist will have injected local anaesthetic into the base of the neck to perform an interscalene block which numbs the nerves in the arm and affords excellent post-operative pain relief. When you wake up from the surgery your arm will feel numb with little movementpossible due to the nerve block and this will last for a number of hours (on average 8-12 hours) following the surgery. The day following surgery the nerve block should have worn off although feeling in the thumb is often the last to recover.
Regular simple anti-inflammatory painkillers are advisable for the first 4-6 weeks and the use of an ice pack on the shoulder may also be helpful to keep the shoulder comfortable for the first 7-10 days. Whilst none of us like taking painkillers for prolonged periods it will take the tendon many weeks to heal and stopping the painkillers too early will often cause the pain to return and make rehabilitation more difficult. It will often take 2-3 months before you will be able to sleep on the operated shoulder comfortably.
Physiotherapy will be organised for you to initially restore your shoulder movement and then from 6-8 weeks post surgery to strengthen the muscle around the joint.
Return to driving usually takes 2 weeks on average and you can return when you feel you can safely use your arm at shoulder height and control objects at this height without inhibition.
Golf and breast stroke swimming can start at 6 weeks following surgery but avoid front crawl swimming for 3 months.
You should be able to return to racquet sports 3 months following your surgery.
You should avoid heavy lifting and repetitive activities for the first 6-8 weeks following the operation as this will aggravate the supraspinatus tendon and cause the shoulder to become painful again. Please avoid repetitive activities above shoulder height for 3 months following your surgery.
In general 80% of patients feel 80% better at approximately 3 months following the surgery. However, some patients are much slower to improve so the speed of your recovery is difficult to predict with certainty. Once the pre-operative symptoms begin to improve then this improvement continues for up to a year following the surgery.
The risks of the operation include infection, a blood collection in the shoulder (haematoma), clot in the leg (DVT), nerve damage, stiffness (post-op frozen shoulder), adverse reaction to the general anaesthetic, incomplete relief of symptoms and recurrence of symptoms. Overall the operation has a success rate (pain resolved and return of good movement and function) of 85-90%.