
Shoulder replacement surgery has been shown to be a highly successful procedure with excellent results for improving symptoms from arthritis. A shoulder replacement is an operation performed to replace the worn out arthritic surfaces of the shoulder joint. 'Arthroplasty' is medical term used to describe the replacement of a joint with an implant. A 'hemiarthroplasty' is the term given to an operation whereby half of the joint is replaced, usually the ball side of the joint (humerus). A 'total shoulder replacement' means that both sides of the shoulder, ie. both the ball and socket, are replaced with implants.
The first shoulder replacement was actually performed in 1892 which was actually more than 25 years before the first hip replacement was attempted. However it wasn't until the 1970s that the use of shoulder replacements became more common. In recent years advances in technology, engineering and understanding of the biomechanics of the shoulder have led to significant advances in shoulder replacement implants.
Originally the implants used to replace the ball side of the joint, the humeral head, would consist of a metal stem inserted down the arm bone (humerus) with a solid metal half sphere attached to the top to replace the arthritic ball part of the joint, the humeral head. If the socket is replaced with an implant as well the ball side being replaced then this is called a 'total shoulder replacement'.
There is debate amongst shoulder surgeons as to whether the socket should be replaced in a shoulder replacement operation. In shoulder replacement surgery the socket component can suffer from loosening or it can wear out much more frequently than the implant that replaces or resurfaces the ball side of the joint. If the socket implant wears out or becomes loose then these are two reasons why patients may need another operation on their shoulder to revise the joint replacement. However, a significant number of patients may continue to have pain from the arthritic socket rubbing against the implant on the ball side of the joint if only the ball side of the joint is replaced. This is a common reason for needing to perform further revision surgery and replace the socket side. Also, recent medical evidence has shown that patients enjoy more pain relief, better range of movement and higher levels of satisfaction with their surgery if both the ball and socket side of the shoulder joint are replaced with a 'total shoulder replacement'. Young patients may not have the socket replaced as due to their young age they are much more likely to wear out the socket implant and need further surgery.
Some patients suffer from wear and tear arthritis of the shoulder which has resulted from the main tendons in the shoulder being torn for a long time. If the tendons in the shoulder are torn then the mechanics of the shoulder alter and the ball, or humeral head of the shoulder, moves incorrectly on the socket causing subsequent arthritis. This type of arthritis is called 'Cuff Tear Arthritis'. Patients who suffer from this often experience severe pain and very limited movement of the shoulder causing severe functional limitations. There is a different type of total shoulder replacement which has been developed specifically for patients who suffer from 'Cuff Tear Arthritis'. A 'reverse geometry' shoulder replacement has been developed whereby the ball and socket of the shoulder are replaced but the implants are 'reversed' whereby the new ball implant is put on the socket side and the socket shaped implant is put on the ball side of the joint. Hence the orientation of the implant is the 'reverse' of the normal shoulder anatomy. When the tendons in the shoulder are torn then the main muscle over the top of the shoulder, the deltoid, is the only muscle which is used to move the patient's shoulder. By 'reversing' the ball and socket configuration of the shoulder replacement the mechanics of the shoulder are altered and the deltoid muscle can work more efficiently. Patients can benefit from a significant improvement in their range of movement and function which is often severely limited with 'cuff tear arthritis'. However, the risks of complications following reverse shoulder replacement are slightly higher than with standard shoulder replacements and therefore a patient must have severe symptoms from 'cuff tear arthritis' and usually be in the older age group to merit this higher risk shoulder replacement.
Operation
A shoulder replacement is performed under a general anaesthetic. The anaesthetist will usually perform an interscalene block, an injection into the lower part of the neck to numb the nerves in the arm, which provides excellent pain relief following the operation . This interscalene block usually lasts for up to 24 hours.
An incision is made over the shoulder and the subscapularis tendon is temporarily detached from the front of the shoulder joint to allow access to the worn out arthritic joint surfaces. The ball and socket of the shoulder, ie. the humeral head and glenoid respectively, are prepared and the shoulder replacement implants are inserted. The subscapularis tendon is then repaired back in place with very strong stitches. The wound is then closed with a stitch. The patient will wake up after the operation with their arm in a sling. This sling is to support the arm which will be numb following the interscalene block and to also rest the shoulder. After the operation a physiotherapist will explain what exercises should be performed. Initially little shoulder movement is allowed although movement of the elbow out of sling is encouraged to prevent elbow stiffness. For the first 6 weeks following surgery it not advised to excessively rotate the arm away from the side of the body (external rotation) as this will put tension on the repair of the subscapularis tendon at the front of the shoulder. It is very important that this subscapularis tendon heals well as it plays a very important role in shoulder function. After 4 weeks the physiotherapist will then wean the patient off the sling and the patient will start more active exercises to improve the range of movement and strength.
The following list indicates the approximate timescale following surgery for patients to return to particular activities:
Return to driving - 6-8 weeks
Return to golf - 3 months
Swimming - breaststroke 6 weeks as tolerated, front crawl minimum 3 months.
Return to work - non-manual work 8 weeks, manual work approximately 6 months.
It can take at least a year following surgery to reach a maximum recovery it terms of range of movement and function.
Risks of shoulder repalcement surgery
The following list indicates the potential complications following a shoulder replacement operation:
General anaesthetic
Implants becoming unstable and dislocating away from each other
Nerve injury
Infection
Blood clot in the leg or lung
Blood collection in shoulder (haematoma) that needs operation to wash out
loosening of the implants
Implant failure
Fracture of a bone in the shoulder
Post-operative rotator cuff tear
Heart attack or stroke
Need for further surgery - for example revision operation to replace implants or repair soft tissues
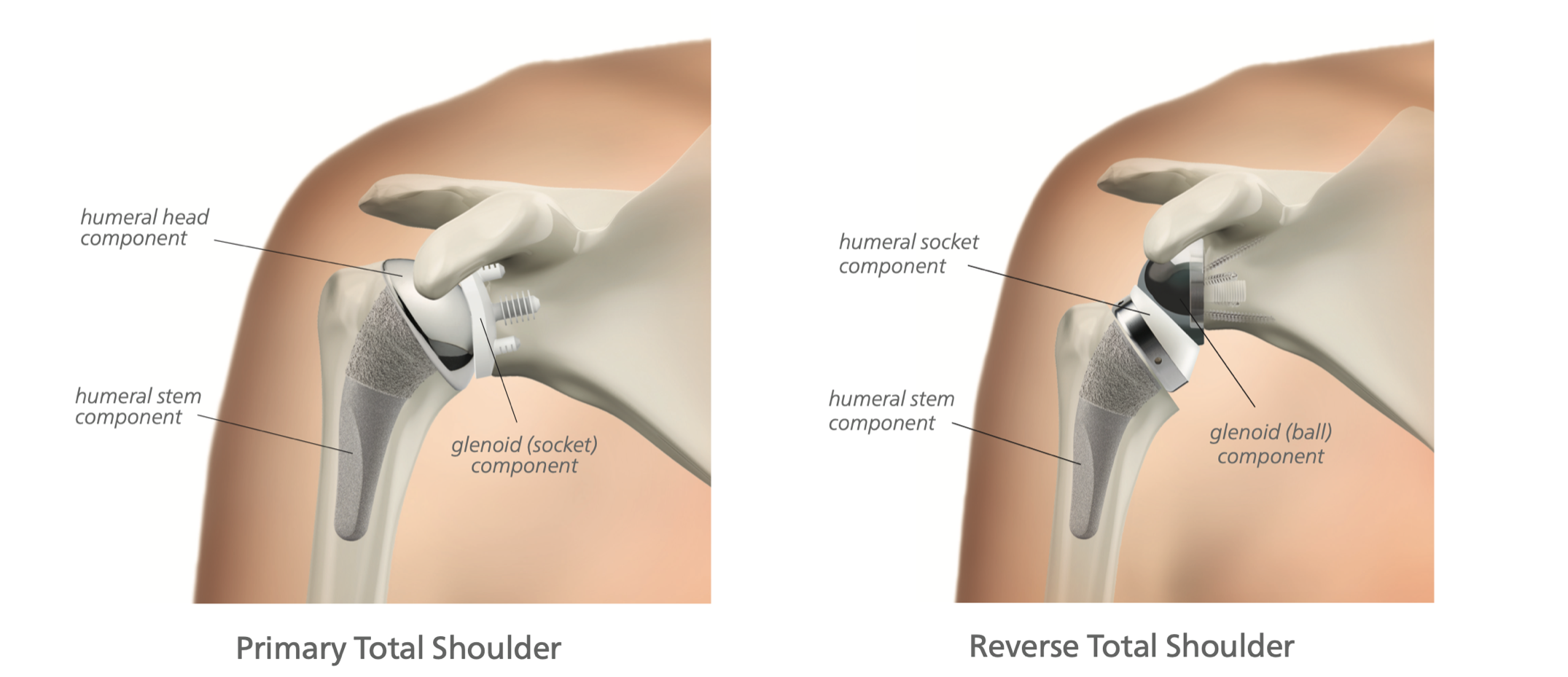
Images courtesy of Wright Medical
REHAB PROTOCOL - TOTAL SHOULDER REPLACEMENT
REHAB PROTOCOL - REVERESE SHOULDER REPLACEMENT
SHOULDER ARTHRITIS
CLINICS
HOME
© 2022 TCSHOULDERELBOWCLINIC CONTACT US CLINICS PROFILE GDPR POLICY